Abstract
Introduction: Infertility is an increasing public health concern in India, affecting approximately 27.5 million couples. Among women, infertility is frequently accompanied by psychosocial stress, societal stigma, and marital conflict, particularly in cultural settings where motherhood is closely linked to feminine identity. Despite technological advances in reproductive medicine, there is limited research examining the combined impact of biological, psychological, and social factors on female infertility and associated health issues. Objectives: This study aims to identify physical, psychological, and relational causes of infertility among women in Tamil Nadu. It also examines the effect of these factors on women's general and mental health. Methods: A purposive sample of 1,200 infertile women aged 18-50 years was selected from fertility centers in Thanjavur and Kumbakonam. Data was collected through structured questionnaires and analyzed using AMOS regression modelling. Fifteen hypotheses were tested to assess relationships among physical health conditions, psychosocial variables, and infertility-related health outcomes. Results: Major physical problems, specifically ovarian cysts (15.2%), thyroid disorders (14.9%), irregular menstruation (10%), and uterine fibroids (8.9%). Significant psychological impacts were observed from couple separation and negative spousal behavior (p < 0.001). Although uterine obstruction, ageing, obesity, and overall health were associated with mental distress, not all showed a direct link to infertility. The model demonstrated good fit indices (CFI = 0.993; RMSEA = 0.035). Conclusion: Infertility in women is a multidimensional issue influenced by physical, psychological, and social factors. Integrating mental health care and relationship counselling into fertility treatment is essential for comprehensive care.
|
Published in
|
Science Journal of Public Health (Volume 13, Issue 5)
|
|
DOI
|
10.11648/j.sjph.20251305.11
|
|
Page(s)
|
244-256 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2025. Published by Science Publishing Group
|
Keywords
Infertility, Psychosomatic Health, Uterine Obstruction, Psychosocial Stress, Regression Analysis, Structural Equation Modeling, Marital Relationship, Hormonal Imbalance, Ovarian Cysts, Thyroid Disorders
1. Introduction
Globally, 10-15% of couples experience infertility. In many cultures, particularly in India, children are seen as vital for family continuity and social rituals. India has 27.5 million infertile couples, a number rising by 5% every two years. According to WHO (2000), infertility rates in India are 3% for primary and 8% for secondary infertility. Infertility is expected to become increasingly common, highlighting the need for support for affected couples. The World Health Organization currently defines infertility as a disability and ‘a disease of the reproductive system defined by the failure to achieve a clinical pregnancy after 12 months or more of regular unprotected sexual intercourse’.
1.1. Review of Literature
India's Total Fertility Rate (TFR) has dropped to 2.0, down from nearly five children per woman in the 1970s (NFHS-5, 2019-21). While most states now have fertility rates below the replacement level of 2.1, Bihar, Meghalaya, and Uttar Pradesh remain higher, especially in rural areas. There are gaps between desired and actual fertility, with many unable to achieve their family planning goals. State-level data shows notable differences: for example, Bihar’s TFR is 3.0 compared to its Total Wanted Fertility Rate (TWFR) of 2.2, while lower-fertility states like Sikkim show smaller gaps. India's adolescent fertility rate is still high at 14.1 per 1,000 women aged 15-19, which poses risks to health, education, and employment.
Female fertility is a broad spectrum of biological, social, psychological, environmental, and lifestyle influences. A significant biological determinant is age, as fertility gradually declines with increasing age due to a reduction in both the quantity and quality of oocytes
| [1] | Anderson SE, Dallal GE, Must A. (2003): Relative weight and race influence average age at menarche: results from two nationally representative surveys of US girls studied 25 years apart. Pediatrics. 111(4 Pt 1): 844-50. |
| [2] | Wallace, WHB and TW Kelsey. (2010): PLoS ONE, 5(1): e8772. |
[1, 2]
. Disorders such as anovulation and fallopian tube obstruction, often due to pelvic inflammatory disease or adhesions, impede fertilization and conception
| [3] | Fauser BC, Devroey P, Yen SS, Gosden R, Crowley WF, Jr., Baird DT, et al. (1999): Minimal ovarian stimulation for IVF: appraisal of potential benefits and drawbacks. Hum Reprod. 14(11): 2681-6. |
| [4] | Sami N, Ali TS, Wasim S, Saleem S. (2012): Risk factors for secondary infertility among women in Karachi, Pakistan. PLoS One. 7(4): e35828. |
[3, 4]
.
Conditions like Polycystic Ovary Syndrome (PCOS) are leading causes of infertility, especially among younger women. PCOS disrupts hormonal balance through elevated androgen levels, resulting in ovulatory dysfunction
| [5] | Barbieri RL. (2001): Am. J. Obstet. Gynecol., 185(5): 1168-1173. |
| [6] | Brassard M, AinMelk Y, Baillargeon JP. (2008): Basic infertility, including polycystic ovary syndrome. Medical Clinics of North America. 92(5): 1163. |
[5, 6]
. Premature ovarian failure, defined by the cessation of ovarian activity before the age of 40, is another critical factor
| [7] | Chatterjee S, Modi D, Maitra A, Kadam S, Patel Z, Gokrall J, et al. (2007): Screening for FOXL2 gene mutations in women with premature ovarian failure: an Indian experience. Reprod Biomed Online. 15(5): 554-60. |
[7]
. Hormonal imbalances, including hyperprolactinemia, thyroid dysfunction, and irregular gonadotropin release, negatively affect ovulation
| [8] | Legro RS. (2007): JAMA, 297(5): 509-519. |
| [9] | Shoupe D, DR Mishell. (1997): Hypoprolactinemia: Diagnosis and treatment. In: Mishell's textbook of Infertility, Contraception and Reproductive Endocrinology. 4th edn. Massachusetts. Blackwell Science, 323-41. |
| [10] | Gohill BC, LA Rosenblum, JD Coplan, JG Kral. (2001): CNS Spectr., 6(7): pp 581-586. |
[8-10]
.
Weight fluctuations are another influential factor. A body mass index (BMI) above 27 kg/m² or significant weight loss has been shown to impair ovarian function and reduce assisted reproductive success
| [11] | Imani B, MJ Eijkemans, ER te Velde, JD Habbema, BC Fauser, (1998): J. Clin. Endocrinol. Metab., 83(7): 2361-2365. |
| [12] | Freundl G, E Godehardt, PA Kern, P Frank-Herrmann, HJ Koubenec, Ch Gnoth (2003): Hum. Reprod., 18(12): 2628-2633. |
[11, 12]
. Obesity increases estrogen levels through adipose tissue, mimicking contraceptive effects and impairing fertility
| [13] | Nelson LR, SE Bulun. (2001): J. Am. Acad. Dermatol., 45(3 Suppl): S116-24. |
| [14] | American Society for Reproductive Medicine (2009): Fertility Fact - Female Risks, 2009. |
[13, 14]
. Conversely, inadequate body fat results in insufficient estrogen, disrupting ovulation and menstruation Nutrition in early life is also linked to reproductive health in adulthood
| [15] | Sloboda DM, Hickey M, Hart R. (2011): Reproduction in females: the role of the early life environment. Hum Reprod Update. 17(2): 210-27. |
[15]
.
Environmental and occupational exposures contribute significantly to infertility risk. Toxins such as pesticides, solvents, glues, and chemical dust are associated with reduced fertility
| [16] | Mendiola J, AM Torres-Cantero, JM Moreno-Grau et al. (2008): Reprod Biomed Online, 16(6): 842-850. |
[16]
. Additionally, chemotherapy drugs such as cyclophosphamide and procarbazine significantly reduce ovarian reserve and hormone levels
| [17] | Rosendahl M, C Andersen, N La Cour Freiesleben, A Juul, K Løssl, A Andersen. (2010): Fertility and sterility 94(1): 156-166. |
| [18] | Brydoy M, SD Fosså, O Dahl, T Bjøro, T. (2007): Acta Oncol,, 46(4): 480-9. |
[17, 18]
.
From a socio-cultural perspective, infertility is often viewed as a woman's issue, leading to stigmatization, social exclusion, and marital instability. The gendered perceptions of infertility highlight the social consequences, such as dowry harassment and divorce faced by women
| [19] | Inhorn MC, Fakih MH. (2005): Arab Americans, African Americans, and infertility: barriers to reproduction and medical care. Fertility and Sterility. 85(4): 844-52. [PubMed: 16580363]. |
| [20] | Unisa, S. (1999): Childlessness in Andhra Pradesh, India: treatment seeking and consequences. Reproductive Health Matters, 7(13): 54-64. |
| [21] | Patel, T. (1994): Fertility Behaviour: Population and Society in a Rajasthan Village. Chapter No. 3. Social and Cultural Context of Fertility. (pp. 74-105), Delhi: Oxford University Press. |
[19-21]
. A study in Andhra Pradesh reported that 14% of husbands of childless women had remarried
| [20] | Unisa, S. (1999): Childlessness in Andhra Pradesh, India: treatment seeking and consequences. Reproductive Health Matters, 7(13): 54-64. |
[20]
, illustrating societal pressures. Many couples are emotionally unprepared to confront infertility, which often results in psychological distress
| [22] | Greil, A. L. (1991): Not yet pregnant: Infertile couples in contemporary America. Rutger University Press, London. |
[22]
.
Cultural expectations link motherhood identity and social status. Failure to conceive can lead to a loss of social standing and emotional suffering
| [23] | Hughes E. G., Collins J, Soliman S, (1995): A Qualitative overview of control trials in endometriosis-associated infertility, Fertil Steril 75(5): 1042-4. |
| [24] | Homans, H. (1982): Pregnancy and Birth as Rites for Two Groups of Women in Britain. In: MacCormack C. P. (ed.), Ethnography of Fertility and Birth, New York Academic Press, New York, 231-268. |
[23, 24]
. Rituals surrounding pregnancy reinforce this association. Women predominantly bear the psychological and physical burdens of infertility and are more likely to face societal discrimination
| [25] | Abbey, A., F. M. Andrew and L. J. Halman, (1991): Gender’s role in response to Infertility. Psychology of Women Quarterly, 15: 295-316. |
| [26] | Runganga, A. O., Sundby, J., and Aggleton, P. (2001): Culture, identity and reproductive failure in Zimbabwe. Sexualities, 4(3), 315-332. |
| [27] | Nene, U., K. Coyaji, V. N. Rao and H. Apte (2002): Infertility: a label of choice in the case of "Sexually Dysfunctional Couple". Paper presented at the International Conference on Infertility in India held in Goa by the IIPS, Mumbai. |
[25-27]
.
Tubal and peritoneal factors-including endometriosis, pelvic adhesions, and infections such as Chlamydia-are significant contributors to infertility
| [28] | Tomassetti C, C Meuleman, A Pexsters et al. (2006): Reprod. Biomed. Online, 13(1): 58-64. |
| [29] | Guven MA, U Dilek, O Pata, S Dilek, P Ciragil. (2007): Arch. Gynecol. Obstet., 276(3): 219-23. |
| [30] | Raga F, C Bauset, J Remohi, F Bonilla-Musoles, C Simón, A Pellicer (1997): Hum. Reprod., 12(10): 2277-81. |
[28-30]
. Endometriosis can create adhesions that interfere with the release and transport of oocytes. Uterine abnormalities such as fibroids, intrauterine septum, and Asherman’s syndrome also compromise implantation and fertility
| [30] | Raga F, C Bauset, J Remohi, F Bonilla-Musoles, C Simón, A Pellicer (1997): Hum. Reprod., 12(10): 2277-81. |
| [31] | Magos A (2002): Reprod. Biomed. Online, 4 Suppl 3: 46-51. |
[30, 31]
.
Thyroid dysfunction is closely associated with menstrual irregularities and infertility. Hypothyroidism and hyperthyroidism can cause ovulatory dysfunction through altered feedback mechanisms involving TSH and prolactin
| [32] | Bjoro T, J Holmen, O Krüger, K Midthjell, K Hunstad, T Schreiner. et al. (2000): Eur J Endocrinol., 143(5): 639-47. |
| [33] | Krassas GE, N Pontikides, T Kaltsas. (1994): Clinical Endocrinology, 40: 641-644. |
[32, 33]
. These hormonal shifts impair follicular development and disrupt the hypothalamus-pituitary axis
| [10] | Gohill BC, LA Rosenblum, JD Coplan, JG Kral. (2001): CNS Spectr., 6(7): pp 581-586. |
[10]
.
Sexually transmitted diseases (STDs) such as gonorrhea, syphilis, chlamydia, and herpes simplex virus can result in infertility through damage to the fallopian tubes and reproductive tract
| [14] | American Society for Reproductive Medicine (2009): Fertility Fact - Female Risks, 2009. |
| [34] | Malik A, Jain S, Hakim S, Shukla I, Rizvi M. (2006): Chlamydia trachomatis infection and female infertility. Indian J Med Res. 123(6): 770-5. |
[14, 34]
. Many STDs are asymptomatic, leading to delayed treatment and increased risk of chronic infection. Pelvic inflammatory disease (PID), often caused by STDs, can result in tubal scarring, ectopic pregnancy, and permanent infertility
| [35] | Senanayake SN. (2008): Med J Aust, 189(8): 456-9. |
[35]
.
Lifestyle factors, including smoking, alcohol consumption, cannabis use, and excessive physical activity, have been documented to impair reproductive function. Smoking alters estrogenic metabolism, reduces uterine blood flow, and affects endometrial receptivity
| [14] | American Society for Reproductive Medicine (2009): Fertility Fact - Female Risks, 2009. |
| [36] | Dechanet C, T Anahory, JC Mathieu Daude, X Quantin, L Reyftmann, S Hamamah, B Hedon, H Dechaud. (2010): Human Reproduction, Update 17(1): 76. |
[14, 36]
. Alcohol intake is linked to increased estrogenic and reduced follicle-stimulating hormone levels, contributing to anovulation
| [37] | Mendelson JH, NK Mello, SK Teoh, and J ellingboe. (1989): Journal of Pharmacology and Experimental Therapeutics, 250, 902-909. |
[37]
. Cannabis may interfere with the endocannabinoid system, thereby impairing fertility
| [38] | Muti P, M Trevisan, A Micheli, V Krogh, G Bolelli, R Sciaryno, HJ Schunemann, and F Berrino. (1998): Cancer Epidemiology Biomarkers and Prevention, 7, 189-193. |
[38]
. Moreover, chronic stress disrupts hormonal balance via the hypothalamic-pituitary-adrenal axis, further influencing ovulatory function
| [39] | Schenker JG, Meirow D, Schenker E. (1992): Stress and human reproduction. Eur J Obstet Gynecol Reprod Biol. 45(1): 1-8. |
| [40] | Taymor ML, Bresnick E. (1979): Emotional stress and infertility. Infertility. 2(1): 39-47. |
[39, 40]
.
Limited healthcare in low socioeconomic areas may lead to underdiagnosis
| [41] | Emily L Silva, Kevin J Lane, Jay Jojo Cheng, Zachary Popp (2024): Polycystic Ovary Syndrome Underdiagnosis Patterns By Individual-Level and Spatial Social Vulnerability Measures, the Journal of Clinical Endocrinology & Metabolism, Dgae 705. |
[41]
. Raising awareness, particularly among women of reproductive age, is vital since many are unaware of Polycystic Ovary Syndrome symptoms, delaying diagnosis and treatment
| [42] | Renae C Fernandez, Vivienne M Moore, Alice R Rumbold, Melissa J Whitrow, Jodie C Avery, Michael J Davies (2021): Diagnosis Delayed: Health Profile Differences Between Women with Undiagnosed Polycystic Ovary Syndrome And Those With A Clinical Diagnosis By Age 35 Years Human Reproduction, Volume 36, Issue 8, Pages 2275-2284. |
[42]
. Urban sedentary lifestyles and diets contribute to higher rates of obesity and metabolic syndrome, increasing Polycystic Ovary Syndrome prevalence. Women with Polycystic Ovary Syndrome face higher risks for obesity, insulin resistance, dyslipidemia, type 2 diabetes
| [43] | H. J. Teede, S. Hutchison, S. Zoungas & C. Meyer (2006): Insulin Resistance, The Metabolic Syndrome, Diabetes, And Cardiovascular Disease Risk In Women with Pcos International Journal of Basic and Clinical Endocrinology, Volume 30, Pages 45-53. |
[43]
, and heart disease
| [44] | Evelyn Talbott, David Guzick, Annette Clerici, Sarah Berga, Katherine Detre, Karl Weimer, And Lewis Kuller (1995): Coronary Heart Disease Risk Factors in Women with Polycystic Ovary Syndrome Arterioscler Thromb Vasc Biol. 15(7): 821-6. |
[44]
. Polycystic Ovary Syndrome also correlates with anxiety, depression, and reduced quality of life, requiring comprehensive care. A Tamil Nadu study reports 8.1% prevalence
| [45] | Mehreen, T. S., Ranjani, H., Kamalesh, R., Ram, U., Anjana, R. M. And Mohan, V. (2021): Prevalence Of Polycystic Ovarian Syndrome Among Adolescents and Young Women In India. Journal of Diabetology, 12(3), 319-325. |
[45]
.
1.2. Study Area
Thanjavur district has been chosen as a study area. According to the 2011 census, it has a population of 2,405,890, a sex ratio of 1,035 females for every 1,000 males, much above the national average of 929. The district had a total of 605,363 households. The area of the district is 3396. 57km2. The population of rural 64.60% and urban 35.40%. At this juncture, present study examines the infertility of reproductive aged women in this region.
1.3. Aim and Objectives
The present study aims to investigate the causes of infertility among reproductive-age women in selected fertility centers in Thanjavur district of Tamil Nadu in India. The objectives are to evaluate the socio-economic and demographic backgrounds of the infertile women in the study area and to analyze the existing causes for infertility of women in this region.
1.4. Methodology
A total of 1200 infertile women, aged 18 to 50, visiting fertility centers in Kumbakonam (600) and Thanjavur (600) towns were selected as respondents for this study through purposive sampling. Each respondent completed a questionnaire during their treatment visits. The questionnaire was drafted in simple Tamil to gather accurate data from infertile respondents, covering socio-economic, demographic, health, and psychological factors. Factor analysis reduced the initial 1200 x 59 dataset to 22 variables, generating a 22 x 22 inter-correlation matrix and a factor loading matrix for assessing variable relationships and variance. Additional analyses included Multiple Regression, AMOS software, and Path Analysis using SEM. These methods examined infertility in women with the observed variables; results showed the path model fit the sample data according to recommended criteria.
2. Results and Findings
2.1. Health Problems and Prevalence of Infertility
A survey of 1,200 women facing infertility (
Table 1) found that 28.1% were under 25 years old, 64.4% were between 26 and 35, 7.3% were 36 to 45, and just 0.5% were older than 46. The average age was 28.43 years. When asked about how long they had unsuccessfully tried to conceive after marriage, 58.3% said it had been up to five years, 32.4% reported between six and ten years, 7.1% between eleven and fifteen years, and 1.6% said more than sixteen years.
Table 1. Selected Variables.
S. No | Variable | Frequency | Percent |
1 | Age of the Respondent |
<25 | 337 | 28.1 |
26-35 | 772 | 64.2 |
36-45 | 86 | 7.3 |
> 46 | 5 | 0.5 |
2 | Not becoming pregnant in the past |
<5 years | 700 | 58.3 |
6-10 years | 390 | 32.5 |
11-15 years | 93 | 7.6 |
16-30 years | 17 | 1.6 |
3 | Body Mass Index | | |
<18.49 Underweight | 50 | 4.2 |
18.50-24.99 Healthy weight | 619 | 51.6 |
25.00-29.99 Overweight | 365 | 30.4 |
30.00-39.99 Obese | 166 | 13.8 |
4 | Husband Health Problems |
No | 910 | 75.8 |
Yes | 290 | 24.2 |
5 | Duration of Treatment |
<3 | 650 | 54.2 |
4-7 | 413 | 34.3 |
8-11 | 102 | 8.5 |
12-16 | 33 | 2.8 |
>17 | 2 | 0.2 |
6 | Number of doctors consulted |
<3 | 951 | 79.2 |
4-7 | 231 | 19.2 |
>8 | 18 | 1.6 |
The study also examined the health status of infertile women, including body mass index. Results showed that 4.2% were underweight, 51.6% had a healthy weight, 30.4% were overweight, and 13.8% were obese.
It wasn’t just the women who faced health issues-24.2% of their husbands also reported health problems and were undergoing fertility treatment alongside their spouses. Most women-54.3%-had been receiving fertility treatments for less than three years, while 34.3% had sought treatment for four to seven years, 8.5% for eight to eleven years, 2.8% for twelve to sixteen years, and 0.2% for more than seventeen years.
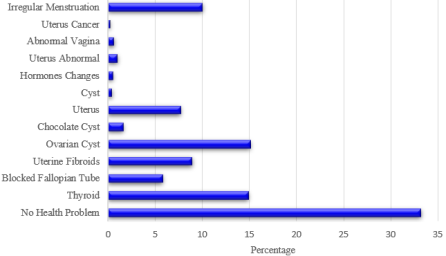
When it came to seeking medical help, 79.2% of the women had consulted fewer than three doctors for fertility issues, 19.2% had seen between four and seven doctors, and 1.6% had visited more than eight. The data revealed that two-thirds of these women (66.7%) identified specific health-related reasons for their infertility, while 33.3% could not pinpoint any known health problems.
Figure 1. Types of Health Problems.
2.2. Ovarian Cyst
Approximately 15.1% of the respondents in this study region were diagnosed with ovarian cysts (
Figure 1). These cysts, generally larger than 2 cm, often develop during the reproductive years and can affect fertility, especially if pathological. In cases of cyst surgical intervention may be required.
2.3. Thyroid Disorders
Thyroid-related issues were observed in 14.9% of participants in this study area. Hypothyroidism can disrupt ovulation due to hormonal imbalances, including elevated prolactin levels. These disruptions contribute significantly to infertility by interfering with egg release and embryo implantation.
2.4. Irregular Menstruation
A total of 10% of women in the data set were reported with irregular menstrual cycles, a key indicator of anovulation. This condition accounts for 30% to 40% of infertility cases, and it is associated with underlying disorders of the thyroid, adrenal, or pituitary glands.
2.5. Uterine Fibroids
Uterine fibroids affected 8.9% of the respondents in this region. These benign tumors, depending on their location and size, may obstruct the fallopian tubes or interfere with the uterine cavity, impacting implantation and leading to infertility.
2.6. Uterine Structural Issues
The data set reveals that the Uterine abnormalities were cited by 7.7% of the women. Though a tilted uterus is not typically problematic, structural anomalies like a septate or bicornuate uterus can hinder the ability to carry a pregnancy to term or prevent conception altogether.
2.7. Blocked Fallopian Tubes
Fallopian tube blockages were observed among the infertile women in 5.8% of respondents. This obstruction can prevent the meeting of the ovum and sperm, rendering fertilization impossible and causing what is termed as tubal ligation infertility.
2.8. Endometriosis / Chocolate Cyst
Endometriosis, leading to chocolate cysts, was reported by 1.6% of women. The condition is associated with inflammation, pelvic pain, and adhesions, all of which can impair reproductive function and egg quality.
2.9. Uterine Abnormalities
One per cent of participants were found to have congenital uterine abnormalities, such as a bicornuate or arcuate uterus. These structural issues can increase the risk of miscarriage and complications during pregnancy.
2.10. Vaginal Abnormalities
Abnormal vaginal conditions, including bacterial vaginosis, affected 0.6% of respondents. This imbalance in vaginal flora may result in increased susceptibility to infections and inflammation that adversely affect fertility.
2.11. Hormonal Imbalance
Hormonal disturbances were identified in 0.5% of cases. Causes include thyroid, pituitary, and hypothalamic dysfunction, overproduction of prolactin, or conditions such as PCOS. These issues disrupt ovulation and create challenges in conception.
2.12. Ovarian Cysts (Non-endometriotic)
A minority (0.4%) of women had benign ovarian cysts, such as dermoid cysts or cystadenomas. While not all cyst types influence fertility, certain forms like endometriomas or cysts associated with PCOS can interfere with reproductive function.
2.13. Uterine Cancer
Uterine or ovarian cancer, though less frequent (0.2%), can necessitate surgical removal of reproductive organs, thereby eliminating fertility. Late diagnosis is common, and contributing factors include genetics, obesity, and infertility treatments.
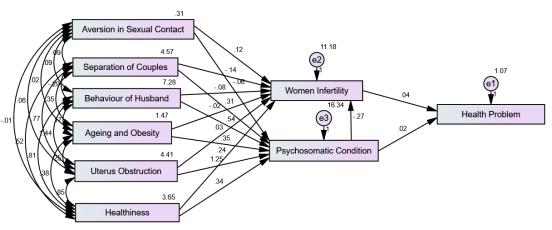
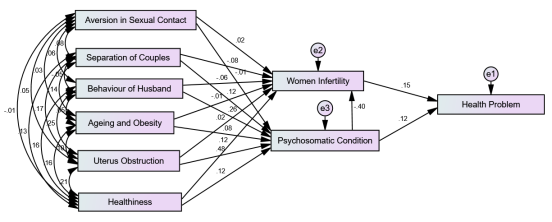
3. Discussion
The above-mentioned physical problems are affecting the pregnancies of women. However, there are some other factors, specifically age, obesity, health issues and psychological conditions, that directly or indirectly influence the fertility of couples. Hence, the following selected assumptions are tested with a regression measurement model using AMOS to evaluate survey consistency. This approach effectively measures causal relationships (
Figure 2 and 3) and verifies model compatibility
| [46] | Peter T (2011): Adoption of Mobile money technology: Structural Equation Modeling Approach. Eur. J. Bus. Manage. 3(7): 2011. |
[46]
.
Figure 2. Path Model on Infertility among Reproductive Age Women: Unstandardized.
Figure 3. Path Model on Infertility among Reproductive Age Women: Standardized.
Accordingly, the following hypotheses have been formulated to test the theoretical framework.
H1: Couple separation significantly affects infertile women's psychological health.
H2: Husband's behavior significantly impacts infertile women's mental condition.
H3: Ageing and obesity influence the psychological state of infertile women.
H4: Uterine obstruction affects infertile women's psychological well-being.
H5: Overall health significantly impacts infertile women's psychology.
H6: Sexual aversion affects infertile women's psychological state.
H7: Sexual aversion influences female infertility.
H8: Couple separation has a significant effect on female infertility.
H9: Husband's behavior impacts female infertility.
H10: Ageing and obesity affect female infertility.
H11: Uterine obstruction influences female infertility.
H12: General health impacts female infertility.
H13: Psychosomatic condition affects female infertility.
H14: Infertility has a significant impact on women's health issues.
H15: Psychosomatic condition affects women's health problems.
This regression model tests how well the data fits a proposed structure. The Chi-square statistic (p = 0.023) indicates a good fit since p < 0.05. However, with a large sample size (1200 in this study), the Chi-square may show significance even when fit is acceptable
| [47] | Joreskog K, Sorbom D (1993). LISREL 7: User’s Reference Guide. Chicago, IL: Scientific Software International Inc. In: Barbara M Byrne, Structural equation modeling with AMOS, Routledge, Taylor Francis. 2. 76-77. |
[47]
. Despite this, the model is suitable for further interpretation using advanced goodness-of-fit measures
| [48] | Barbara MB (2009). Structural Equation Modelling with AMOS. Basic concepts, applications, and programming. 2nd Edn, Routledge, Taylor & Francis Group, New York. pp. 76-84. |
[48]
. Standard indices such as χ²/df, CFI, RMSEA, NFI, IFI, and TLI were used to evaluate fit.
Table 2 presents these results from AMOS analysis. The following goodness of fit indices indicates an acceptable model for this study
| [49] | Gerbing DW, Anderson JC (1992). Monte Carlo evaluations of goodness of fit indices for structural equation models. Social. Methods Res. 21(2): 132-160. |
[49]
: RMSEA should be 0.08 or lower, CFI should be 0.90 or higher, and NFI should also be 0.90 or higher.
The fit between the collected data and the proposed measurement model was assessed using a Chi-Square Goodness of Fit Index (GFI) test, where a value greater than or equal to 0.9 signifies a good fit
| [50] | Hu LT, Bentler PM (1999). Cut off Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria versus New Alternatives, Struct. Equ. Model. 6(1): 1-55. |
[50]
. In this study (
Table 2), the GFI was 0.997, exceeding the recommended threshold of 0.90, and other indices also demonstrated satisfactory fit: AGFI = 0.980, RFI = 0.932, CFI = 0.993, TLI = 0.959, IFI = 0.993, NFI = 0.989, with χ2/df = 2.447, RMSEA = 0.035
| [51] | Bagozzi RP, Yi Y (1988). On the evaluation of structural equation models. J. Acad. Mark. Sci. 16(1): 74-94. |
[51]
, RMR = 0.009, and PGFI = 0.113. These results collectively indicate a strong overall model fit. The goodness of fit indices confirms the suitability of the structural model, as evidenced by the reported values.
Based on the above-cited hypotheses, the AMOS results show fifteen regression weights and both unstandardized and standardized factor models for each path and its significance (
Table 3). The unstandardized regression coefficient indicates how much the dependent or mediating variable changes per unit increase in the predictor variable. Standardized estimate, standard error (S.E.), and critical ratio (C.R., calculated as estimate divided by S.E.). The P column shows the probability value for the null hypothesis.
Table 2. Fit statistics of the Measurement model.
Sl. No. | Fit statistic | Recommended | Obtained |
1 | Chi Square | - | 14.683 |
2 | df | - | 6 |
3 | Chi-Square significance | P< =0.05 | 0.023 |
4 | Chi Square ⁄df | <5.0 | 2.447 |
5 | Goodness of Fit Index (GFI) | >0.9 | 0.997 |
6 | Adjusted Goodness of Fit Index (AGFI) | >0.9 | 0.980 |
7 | Normated Fit Index (NFI) | >0.9 | 0.989 |
8 | Relative Fit Index (RFI) | >0.9 | 0.932 |
9 | Comparative Fit index (CFI) | >0.9 | 0.993 |
10 | Tucker Lewis Index (TLI) | >0.9 | 0.959 |
11 | Incremental Fit Index (IFI) | Approaches 1 | 0.993 |
12 | Root means square error of approximation (RMSEA) | <0.05 | 0.035 |
13 | Root Mean Square Residual (RMR) | <0.02 | 0.009 |
14 | Parsimony goodness-of-fit index (PGFI) | <5.0 | 0.133 |
3.1. H1: Couple Separation Significantly Affects Infertile Women's Psychological Health
The findings indicate that increased separation between couples significantly affects the psychological condition of infertile women. A one-unit rise in separation corresponds to a 0.306-unit increase in psychological distress, with a standard error of 0.057. The resulting z-value is 5.411, which is statistically significant at the 0.001 level. This confirms that relationship disruption contributes substantially to psychological difficulties among women facing infertility.
3.2. H2: Husband's Behavior Significantly Impacts Infertile Women's Mental Condition
The analysis shows that the husband’s behavior significantly influences the psychological condition of infertile women. A one-unit improvement in behavior leads to a 0.539 unit increase in psychological well-being. The standard error is 0.045, with a z-value of 11.880, indicating significance at the 0.001 level. These results affirm that supportive spousal behavior is a crucial determinant of emotional stability among women experiencing infertility.
3.3. H3: Ageing and Obesity Influence the Psychological State of Infertile Women
Ageing and obesity were found to exert a meaningful influence on psychological status. A one-unit increase in this combined factor results in a 0.352-unit rise in psychological condition, with a standard error of 0.099. The calculated z-value of 3.570 is statistically significant at the 0.001 level. This validates that age-related and weight-related challenges contribute to heightened psychological distress in infertile women.
3.4. H4: Uterine Obstruction Affects Infertile Women's Psychological Well-being
Uterine obstruction was identified as having the strongest effect among the tested variables. A one-unit increase in obstruction corresponds to a 1.245-unit rise in psychological disturbance. The standard error is 0.059, yielding a z-value of 20.968. This highly significant result (p < 0.001) confirms that physical reproductive impediments substantially impact the mental health of infertile women.
3.5. H5: Overall Health Significantly Impacts Infertile Women's Psychology
A significant positive relationship was observed between healthiness and psychological condition. A one-unit increase in health status is linked to a 0.338-unit improvement in psychological well-being, with a standard error of 0.064. The z-value of 5.288 signifies strong statistical significance (p < 0.001), indicating that overall physical health is an important contributor to better psychological outcomes among infertile women.
3.6. H6: Sexual Aversion Affects Infertile Women's Psychological State
In terms of psychological condition, aversion to sexual contact showed no significant relationship; a one-unit increase in aversion led to only a 0.064-unit decrease, with a high standard error and p-value above 0.05. Additionally, the variables "husband not interested in intercourse" and "self not interested in intercourse" were positively associated, reported by 1.1% and 2.0% of respondents, respectively. Together, these findings indicate that sexual contact is identified as a factor contributing to unproductiveness among women in this study area.
Table 3. Regression Weights for Every Path and Its Significance.
Sl. No. | Construct | Path | Construct | Unstandardized co-efficient | S.E. | Standardized co-efficient | C.R. | P | Label |
1 | Psychosomatic Condition | <--- | Separation of Couples | 0.306 | 0.057 | 0.119 | 5.411 | 0.001** | Significant |
2 | Psychosomatic Condition | <--- | Behavior of Husband | 0.539 | 0.045 | 0.264 | 11.880 | 0.001** | Significant |
3 | Psychosomatic Condition | <--- | Ageing and Obesity | 0.352 | 0.099 | 0.077 | 3.570 | 0.001** | Significant |
4 | Psychosomatic Condition | <--- | Uterus Obstruction | 1.245 | 0.059 | 0.475 | 20.968 | 0.001** | Significant |
5 | Psychosomatic Condition | <--- | Healthiness | 0.338 | 0.064 | 0.117 | 5.288 | 0.001** | Significant |
6 | Psychosomatic Condition | <--- | Aversion in Sexual Contact | -0.064 | 0.210 | -0.006 | -0.302 | 0.762 | Not Significant |
7 | Infertility | <--- | Aversion in Sexual Contact | 0.118 | 0.174 | 0.018 | 0.678 | 0.498 | Not Significant |
8 | Infertility | <--- | Separation of Couples | -0.136 | 0.047 | -0.079 | -2.878 | 0.004** | Significant |
9 | Infertility | <--- | Behavior of Husband | -0.081 | 0.040 | -0.060 | -2.053 | 0.040* | Significant |
10 | Infertility | <--- | Ageing and Obesity | -0.017 | 0.082 | -0.006 | -0.213 | 0.831 | Not Significant |
11 | Infertility | <--- | Uterus Obstruction | 0.030 | 0.057 | 0.017 | 0.527 | 0.598 | Not Significant |
12 | Infertility | <--- | Healthiness | 0.237 | 0.053 | 0.123 | 4.440 | 0.001** | Significant |
13 | Infertility | <--- | Psychosomatic Condition | -0.269 | 0.024 | -0.402 | -11.270 | 0.001** | Significant |
14 | Health Problem | <--- | Infertility | 0.044 | 0.009 | 0.154 | 4.969 | 0.001** | Significant |
15 | Health Problem | <--- | Psychosomatic Condition | 0.023 | 0.006 | 0.122 | 3.909 | 0.001** | Significant |
3.7. H7: Sexual Aversion Influences Female Infertility
Similarly, no significant association was found between aversion to sexual contact and infertility. Although a one-unit increase in aversion yields a 0.118-unit rise in infertility, the standard error of 0.174 results in a z-value of 0.678. Since this value does not meet the threshold for significance (p > 0.05), the hypothesis of a relationship between aversion to sexual contact and infertility is rejected. The data also include two health-related variables: eggs not developing due to hormonal issues and experiences of miscarriage or abortion. Among respondents, 24.8% reported eggs not developing because of hormone-related problems, while 28.3% indicated frequent abortions. These results suggest that, while aversion to sexual contact shows no significant link to infertility, other health factors may influence women's fertility in this region.
3.8. H8: Couple Separation Has a Significant Effect on Female Infertility
The analysis indicates that partner separation significantly decreases infertility, with a one-unit increase in separation associated with a 0.136-unit decrease in infertility (standard error: 0.047, z = -2.878, p < 0.01). This effect may result from reduced sexual activity or other factors related to relationship instability. Two variables, husbands working away from home and infrequent meetings, loaded highly on this factor. In the study, 20.9% of respondents’ husbands worked elsewhere, meeting only during weekly or monthly leave, highlighting separation as a primary contributor to infertility.
3.9. H9: Husband's Behavior Impacts Female Infertility
The behavior of the husband significantly influences infertility outcomes. A one-unit improvement in behavior is associated with a 0.081-unit reduction in infertility. The standard error is 0.040, and the z-value of -2.053 confirms statistical significance at the 0.05 level. This underscores the role of spousal conduct in reproductive health.
3.10. H10: Ageing and Obesity Affect Female Infertility
In this dataset, the combined impact of aging and obesity does not significantly affect infertility (z = -0.213, p > 0.05). A one-unit increase is associated with a 0.017 decrease in infertility, with a standard error of 0.082. Although age and obesity are recorded as reasons for infertility, this study finds no significant combined effect on women’s fertility in the area studied.
3.11. H11: Uterine Obstruction Influences Female Infertility
The analysis shows no significant link between uterine obstruction and infertility (z = 0.527, p > 0.05). Endometrium, fibroid, and cyst factors loaded positively, while white discharge loaded negatively. Tumours or fluid block ovaries in 28.5% and 31.6% of respondents, respectively; 18.1% experience white discharge. The study indicates that tumour growth and fluid secretion are key contributors to infertility in this region.
3.12. H12: General Health Condition Impacts Female Infertility
A statistically significant relationship was identified between healthiness and infertility, with each one-unit increase in healthiness corresponding to a 0.237-unit increase in infertility (standard error = 0.053). The z-value of 4.440 demonstrates significance at the 0.001 level. This outcome may be affected by interactions involving perceived health, reproductive factors, or stress. Health is connected to various activities and can influence pregnancy outcomes. Two related variables investigated were eggs not developing due to hormone issues and miscarriage/abortion: 24.8 per cent of respondents reported problems with egg development associated with hormonal factors, while 28.3 per cent reported frequent miscarriages or abortions. These results indicate that healthiness is a variable associated with fertility among women in the population studied.
3.13. H13: Psychosomatic Condition Affects Female Infertility
Psychosomatic condition was found to have a strong negative association with infertility. An increase of one unit in psychosomatic distress results in a 0.269 unit decrease in infertility. The standard error is 0.024, yielding a highly significant z-value of -11.270 (p < 0.001). This suggests that mental and emotional disturbances may play a significant role in reproductive difficulties.
3.14. H14: Infertility Has a Significant Impact on Women's Health Issues
The findings confirm that infertility significantly contributes to broader health issues among women. A one-unit increase in infertility is associated with a 0.044-unit increase in health problems. With a standard error of 0.009 and a z-value of 4.969, this relationship is statistically significant at the 0.001 level, highlighting the cascading effects of infertility on general health.
3.15. H15: Psychosomatic Condition Affects Women's Health Problems
Psychosomatic factors were also shown to significantly influence women's health issues. A one-unit increase in psychosomatic symptoms corresponds to a 0.023-unit rise in health problems. The standard error is 0.006, with a z-value of 3.909, confirming significance at the 0.001 level. This demonstrates the strong interplay between mental health and physical well-being in the context of infertility.
4. Conclusion
The present study systematically examined the influence of various psychological and physiological factors on infertility and health conditions among women. The findings highlight that relational variables such as separation between couples and the behavior of husbands play a critical role in shaping the psychological well-being of infertile women. Specifically, emotional detachment and unsupportive partner behavior were strongly associated with increased psychological distress. Additionally, factors such as ageing, obesity, and uterine obstruction were also found to significantly affect mental health, though not all showed a direct impact on infertility itself.
While healthiness was shown to improve psychological condition, it exhibited a paradoxical relationship with infertility, suggesting the complexity of health perceptions and reproductive capacity. Importantly, psychosomatic conditions emerged as a significant predictor of both infertility and broader health problems, underscoring the intertwined nature of emotional and physical health.
The study also revealed that infertility has a consequential effect on women's overall health status, further reinforcing the need to address reproductive challenges not merely as isolated medical conditions but as issues that impact multiple dimensions of women’s lives. Though some hypotheses, such as those related to sexual aversion, did not yield statistically significant results, the broader pattern of findings affirms that infertility is influenced by psychosocial, behavioral, and biological factors.
5. Research Gaps
Despite the depth of analysis provided in the current study, several critical research gaps remain: While the manuscript acknowledges male infertility, it focuses predominantly on women. The sociocultural context in India often attributes infertility to women, thereby marginalizing male factors. Comprehensive studies incorporating male physiological and psychological parameters are lacking. The finding that better health is associated with increased infertility contradicts established biomedical expectations.
This paradoxical relationship requires further investigation to understand potential underlying mechanisms, including psychosomatic influences and subjective health perceptions. The impact of sexual aversion on infertility and psychological health was statistically insignificant. However, given the sensitive nature of sexual health, the responses may be influenced by social desirability bias. More nuanced, qualitative research methods are needed to capture this complex dimension. Although briefly discussed in the literature review, environmental toxins and occupational hazards were not empirically examined in the study.
These remain underexplored despite growing evidence of their impact on reproductive health. The cross-sectional design of the study limits understanding of temporal changes in infertility and associated psychosocial outcomes. A longitudinal framework would provide more insight into causal relationships and treatment trajectories. The study does not differentiate the outcomes based on treatment types or assess how socio-economic status affects access and response to infertility treatments.
6. Implementation
To effectively translate the findings of this research into practical applications within clinical and community health settings, several strategies can be considered.
The study points out that fertility clinics should adopt a multidisciplinary approach. This means integrating not only specialists in gynecology and endocrinology but also providing access to psychological counselling and relationship therapy. Addressing psychosomatic issues is crucial, as the role of the husband’s behavior and the impact of couple separation is significant. Therefore, it’s important to implement targeted counselling and awareness initiatives that engage both partners, promoting supportive relationships throughout the infertility treatment process.
The research also highlights the need for regular reproductive health screenings, particularly in rural and semi-urban areas, to catch age-related and obesity-related risks early. Special focus should be placed on women in their late twenties and older, since this is when fertility begins to decline more sharply. Government agencies must work to spread reliable, evidence-based information regarding infertility causes, utilizing culturally relevant methods to break down stigma and encourage couples to seek help.
Furthermore, it's vital to establish standardized tools for psychosomatic assessments in fertility clinics. This would enable regular monitoring of patients' mental health and help predict their health outcomes. Finally, leveraging findings from regression analyses can support advocacy efforts for infertility to be recognized in public health policy as both a medical and psychological issue, which deserves funding and insurance coverage.
7. Recommendations
To advance our understanding of infertility and improve treatment outcomes, we must implement the following recommendations. Future research should embrace integrative models that consider both partners' physical and mental health within the fertility context. This approach will help identify root causes and assess intervention effectiveness, ultimately guiding clinical practices. Conducting studies across various Indian states and socio-economic groups will provide key insights into the determinants and impacts.
It is also vital to recognize the influence of cultural norms on infertility perceptions. Exploring indigenous health beliefs can lead to culturally resonant care models. Additionally, mental health services should be integrated into treatment protocols, and all fertility centers must provide access to trained counsellors. We need to raise awareness and destigmatize male infertility to promote equitable diagnostic procedures and ease psychological burdens on women. Finally, developing mobile apps to deliver reproductive health education and support services is essential, particularly for underserved rural populations.
8. Ethical Considerations
This study followed ethical standards for research involving human participants and received approval (Ref: Bharathidasan University, Tiruchirappalli, Tamil Nadu/15714/Geography/Date: 03/10/2017) from the Institutional Ethics Committee of Government Arts College (Autonomous), Kumbakonam, before data collection. Participants were informed about the study's purpose and provided written consent. Participation was voluntary, and we ensured strict confidentiality by anonymizing data and not recording personal identifiers.
9. Limitations of the Study
This study presents a strong, large sample size and thorough statistical analysis, yet it has notable limitations. Its reliance on cross-sectional data restricts the ability to establish causal relationships between psychosocial factors and infertility outcomes, making longitudinal research essential for deeper insights. Additionally, the data were collected from fertility clinics in just two urban centers in Tamil Nadu, which may not represent the experiences of rural populations or those who do not seek formal treatment. Focusing solely on female respondents also overlooks significant male infertility factors.
Moreover, sensitive topics like sexual aversion and psychological distress may have been underreported due to social desirability or stigma. Finally, the absence of a thorough examination of environmental and occupational risks limits the study’s comprehensiveness. Addressing these aspects could greatly enhance our understanding of infertility.
Abbreviations
AMOS | Analysis of Moment Structure |
NFHS | National Family Health Survey |
SEM | Structural Equation Model |
PCOS | Polycystic Ovary Syndrome |
Acknowledgments
Compiled and analyzed by the author(s) based on primary data collected in Thanjavur District.
Author Contributions
Vadivel Sivalingam: Conceptualization, Data curation, Formal Analysis, Methodology, Project administration, Software, Supervision, Validation, Writing – original draft, Writing – review & editing
Shanmugam Muruganandham: Conceptualization, Data curation, Investigation, Methodology, Resources, Validation, Visualization, Writing – review & editing
Sankar Karuppaiyan: Conceptualization, Formal Analysis, Investigation, Resources, Supervision, Validation, Writing – original draft
Mayakannan Ayyanar: Data curation, Formal Analysis, Investigation, Methodology, Software, Validation, Visualization
Ethics Approval
This study was conducted according to ethical standards and guidelines. Approval was obtained from the relevant institutional review board (IRB: Ref: Bharathidasan University, Tiruchirappalli, Tamil Nadu/15714/Geography/Date: 03/10/2017) before the commencement of the research. Informed consent was obtained from all participants involved in the study, ensuring their voluntary participation and confidentiality of their data. The research adhered to ethical principles such as respect for persons, beneficence, and justice, ensuring that the rights and welfare of the participants were protected throughout the study.
Consent to Participate
Informed consent was obtained from all individual participants’ parents or legal guardians included in the study.
Consent for Publication
Not applicable, as the manuscript does not contain any personal identifiable information or images.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Anderson SE, Dallal GE, Must A. (2003): Relative weight and race influence average age at menarche: results from two nationally representative surveys of US girls studied 25 years apart. Pediatrics. 111(4 Pt 1): 844-50.
|
| [2] |
Wallace, WHB and TW Kelsey. (2010): PLoS ONE, 5(1): e8772.
|
| [3] |
Fauser BC, Devroey P, Yen SS, Gosden R, Crowley WF, Jr., Baird DT, et al. (1999): Minimal ovarian stimulation for IVF: appraisal of potential benefits and drawbacks. Hum Reprod. 14(11): 2681-6.
|
| [4] |
Sami N, Ali TS, Wasim S, Saleem S. (2012): Risk factors for secondary infertility among women in Karachi, Pakistan. PLoS One. 7(4): e35828.
|
| [5] |
Barbieri RL. (2001): Am. J. Obstet. Gynecol., 185(5): 1168-1173.
|
| [6] |
Brassard M, AinMelk Y, Baillargeon JP. (2008): Basic infertility, including polycystic ovary syndrome. Medical Clinics of North America. 92(5): 1163.
|
| [7] |
Chatterjee S, Modi D, Maitra A, Kadam S, Patel Z, Gokrall J, et al. (2007): Screening for FOXL2 gene mutations in women with premature ovarian failure: an Indian experience. Reprod Biomed Online. 15(5): 554-60.
|
| [8] |
Legro RS. (2007): JAMA, 297(5): 509-519.
|
| [9] |
Shoupe D, DR Mishell. (1997): Hypoprolactinemia: Diagnosis and treatment. In: Mishell's textbook of Infertility, Contraception and Reproductive Endocrinology. 4th edn. Massachusetts. Blackwell Science, 323-41.
|
| [10] |
Gohill BC, LA Rosenblum, JD Coplan, JG Kral. (2001): CNS Spectr., 6(7): pp 581-586.
|
| [11] |
Imani B, MJ Eijkemans, ER te Velde, JD Habbema, BC Fauser, (1998): J. Clin. Endocrinol. Metab., 83(7): 2361-2365.
|
| [12] |
Freundl G, E Godehardt, PA Kern, P Frank-Herrmann, HJ Koubenec, Ch Gnoth (2003): Hum. Reprod., 18(12): 2628-2633.
|
| [13] |
Nelson LR, SE Bulun. (2001): J. Am. Acad. Dermatol., 45(3 Suppl): S116-24.
|
| [14] |
American Society for Reproductive Medicine (2009): Fertility Fact - Female Risks, 2009.
|
| [15] |
Sloboda DM, Hickey M, Hart R. (2011): Reproduction in females: the role of the early life environment. Hum Reprod Update. 17(2): 210-27.
|
| [16] |
Mendiola J, AM Torres-Cantero, JM Moreno-Grau et al. (2008): Reprod Biomed Online, 16(6): 842-850.
|
| [17] |
Rosendahl M, C Andersen, N La Cour Freiesleben, A Juul, K Løssl, A Andersen. (2010): Fertility and sterility 94(1): 156-166.
|
| [18] |
Brydoy M, SD Fosså, O Dahl, T Bjøro, T. (2007): Acta Oncol,, 46(4): 480-9.
|
| [19] |
Inhorn MC, Fakih MH. (2005): Arab Americans, African Americans, and infertility: barriers to reproduction and medical care. Fertility and Sterility. 85(4): 844-52. [PubMed: 16580363].
|
| [20] |
Unisa, S. (1999): Childlessness in Andhra Pradesh, India: treatment seeking and consequences. Reproductive Health Matters, 7(13): 54-64.
|
| [21] |
Patel, T. (1994): Fertility Behaviour: Population and Society in a Rajasthan Village. Chapter No. 3. Social and Cultural Context of Fertility. (pp. 74-105), Delhi: Oxford University Press.
|
| [22] |
Greil, A. L. (1991): Not yet pregnant: Infertile couples in contemporary America. Rutger University Press, London.
|
| [23] |
Hughes E. G., Collins J, Soliman S, (1995): A Qualitative overview of control trials in endometriosis-associated infertility, Fertil Steril 75(5): 1042-4.
|
| [24] |
Homans, H. (1982): Pregnancy and Birth as Rites for Two Groups of Women in Britain. In: MacCormack C. P. (ed.), Ethnography of Fertility and Birth, New York Academic Press, New York, 231-268.
|
| [25] |
Abbey, A., F. M. Andrew and L. J. Halman, (1991): Gender’s role in response to Infertility. Psychology of Women Quarterly, 15: 295-316.
|
| [26] |
Runganga, A. O., Sundby, J., and Aggleton, P. (2001): Culture, identity and reproductive failure in Zimbabwe. Sexualities, 4(3), 315-332.
|
| [27] |
Nene, U., K. Coyaji, V. N. Rao and H. Apte (2002): Infertility: a label of choice in the case of "Sexually Dysfunctional Couple". Paper presented at the International Conference on Infertility in India held in Goa by the IIPS, Mumbai.
|
| [28] |
Tomassetti C, C Meuleman, A Pexsters et al. (2006): Reprod. Biomed. Online, 13(1): 58-64.
|
| [29] |
Guven MA, U Dilek, O Pata, S Dilek, P Ciragil. (2007): Arch. Gynecol. Obstet., 276(3): 219-23.
|
| [30] |
Raga F, C Bauset, J Remohi, F Bonilla-Musoles, C Simón, A Pellicer (1997): Hum. Reprod., 12(10): 2277-81.
|
| [31] |
Magos A (2002): Reprod. Biomed. Online, 4 Suppl 3: 46-51.
|
| [32] |
Bjoro T, J Holmen, O Krüger, K Midthjell, K Hunstad, T Schreiner. et al. (2000): Eur J Endocrinol., 143(5): 639-47.
|
| [33] |
Krassas GE, N Pontikides, T Kaltsas. (1994): Clinical Endocrinology, 40: 641-644.
|
| [34] |
Malik A, Jain S, Hakim S, Shukla I, Rizvi M. (2006): Chlamydia trachomatis infection and female infertility. Indian J Med Res. 123(6): 770-5.
|
| [35] |
Senanayake SN. (2008): Med J Aust, 189(8): 456-9.
|
| [36] |
Dechanet C, T Anahory, JC Mathieu Daude, X Quantin, L Reyftmann, S Hamamah, B Hedon, H Dechaud. (2010): Human Reproduction, Update 17(1): 76.
|
| [37] |
Mendelson JH, NK Mello, SK Teoh, and J ellingboe. (1989): Journal of Pharmacology and Experimental Therapeutics, 250, 902-909.
|
| [38] |
Muti P, M Trevisan, A Micheli, V Krogh, G Bolelli, R Sciaryno, HJ Schunemann, and F Berrino. (1998): Cancer Epidemiology Biomarkers and Prevention, 7, 189-193.
|
| [39] |
Schenker JG, Meirow D, Schenker E. (1992): Stress and human reproduction. Eur J Obstet Gynecol Reprod Biol. 45(1): 1-8.
|
| [40] |
Taymor ML, Bresnick E. (1979): Emotional stress and infertility. Infertility. 2(1): 39-47.
|
| [41] |
Emily L Silva, Kevin J Lane, Jay Jojo Cheng, Zachary Popp (2024): Polycystic Ovary Syndrome Underdiagnosis Patterns By Individual-Level and Spatial Social Vulnerability Measures, the Journal of Clinical Endocrinology & Metabolism, Dgae 705.
|
| [42] |
Renae C Fernandez, Vivienne M Moore, Alice R Rumbold, Melissa J Whitrow, Jodie C Avery, Michael J Davies (2021): Diagnosis Delayed: Health Profile Differences Between Women with Undiagnosed Polycystic Ovary Syndrome And Those With A Clinical Diagnosis By Age 35 Years Human Reproduction, Volume 36, Issue 8, Pages 2275-2284.
|
| [43] |
H. J. Teede, S. Hutchison, S. Zoungas & C. Meyer (2006): Insulin Resistance, The Metabolic Syndrome, Diabetes, And Cardiovascular Disease Risk In Women with Pcos International Journal of Basic and Clinical Endocrinology, Volume 30, Pages 45-53.
|
| [44] |
Evelyn Talbott, David Guzick, Annette Clerici, Sarah Berga, Katherine Detre, Karl Weimer, And Lewis Kuller (1995): Coronary Heart Disease Risk Factors in Women with Polycystic Ovary Syndrome Arterioscler Thromb Vasc Biol. 15(7): 821-6.
|
| [45] |
Mehreen, T. S., Ranjani, H., Kamalesh, R., Ram, U., Anjana, R. M. And Mohan, V. (2021): Prevalence Of Polycystic Ovarian Syndrome Among Adolescents and Young Women In India. Journal of Diabetology, 12(3), 319-325.
|
| [46] |
Peter T (2011): Adoption of Mobile money technology: Structural Equation Modeling Approach. Eur. J. Bus. Manage. 3(7): 2011.
|
| [47] |
Joreskog K, Sorbom D (1993). LISREL 7: User’s Reference Guide. Chicago, IL: Scientific Software International Inc. In: Barbara M Byrne, Structural equation modeling with AMOS, Routledge, Taylor Francis. 2. 76-77.
|
| [48] |
Barbara MB (2009). Structural Equation Modelling with AMOS. Basic concepts, applications, and programming. 2nd Edn, Routledge, Taylor & Francis Group, New York. pp. 76-84.
|
| [49] |
Gerbing DW, Anderson JC (1992). Monte Carlo evaluations of goodness of fit indices for structural equation models. Social. Methods Res. 21(2): 132-160.
|
| [50] |
Hu LT, Bentler PM (1999). Cut off Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria versus New Alternatives, Struct. Equ. Model. 6(1): 1-55.
|
| [51] |
Bagozzi RP, Yi Y (1988). On the evaluation of structural equation models. J. Acad. Mark. Sci. 16(1): 74-94.
|
Cite This Article
-
APA Style
Sivalingam, V., Muruganandham, S., Karuppaiyan, S., Ayyanar, M. (2025). Multifactorial Analysis of Infertility and Women's Health: Evidence from Fertility Clinics in Tamil Nadu, India. Science Journal of Public Health, 13(5), 244-256. https://doi.org/10.11648/j.sjph.20251305.11
 Copy
|
Copy
|
 Download
Download
ACS Style
Sivalingam, V.; Muruganandham, S.; Karuppaiyan, S.; Ayyanar, M. Multifactorial Analysis of Infertility and Women's Health: Evidence from Fertility Clinics in Tamil Nadu, India. Sci. J. Public Health 2025, 13(5), 244-256. doi: 10.11648/j.sjph.20251305.11
Copy
|
Download
AMA Style
Sivalingam V, Muruganandham S, Karuppaiyan S, Ayyanar M. Multifactorial Analysis of Infertility and Women's Health: Evidence from Fertility Clinics in Tamil Nadu, India. Sci J Public Health. 2025;13(5):244-256. doi: 10.11648/j.sjph.20251305.11
Copy
|
Download
-
@article{10.11648/j.sjph.20251305.11,
author = {Vadivel Sivalingam and Shanmugam Muruganandham and Sankar Karuppaiyan and Mayakannan Ayyanar},
title = {Multifactorial Analysis of Infertility and Women's Health: Evidence from Fertility Clinics in Tamil Nadu, India
},
journal = {Science Journal of Public Health},
volume = {13},
number = {5},
pages = {244-256},
doi = {10.11648/j.sjph.20251305.11},
url = {https://doi.org/10.11648/j.sjph.20251305.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.sjph.20251305.11},
abstract = {Introduction: Infertility is an increasing public health concern in India, affecting approximately 27.5 million couples. Among women, infertility is frequently accompanied by psychosocial stress, societal stigma, and marital conflict, particularly in cultural settings where motherhood is closely linked to feminine identity. Despite technological advances in reproductive medicine, there is limited research examining the combined impact of biological, psychological, and social factors on female infertility and associated health issues. Objectives: This study aims to identify physical, psychological, and relational causes of infertility among women in Tamil Nadu. It also examines the effect of these factors on women's general and mental health. Methods: A purposive sample of 1,200 infertile women aged 18-50 years was selected from fertility centers in Thanjavur and Kumbakonam. Data was collected through structured questionnaires and analyzed using AMOS regression modelling. Fifteen hypotheses were tested to assess relationships among physical health conditions, psychosocial variables, and infertility-related health outcomes. Results: Major physical problems, specifically ovarian cysts (15.2%), thyroid disorders (14.9%), irregular menstruation (10%), and uterine fibroids (8.9%). Significant psychological impacts were observed from couple separation and negative spousal behavior (p Conclusion: Infertility in women is a multidimensional issue influenced by physical, psychological, and social factors. Integrating mental health care and relationship counselling into fertility treatment is essential for comprehensive care.
},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Multifactorial Analysis of Infertility and Women's Health: Evidence from Fertility Clinics in Tamil Nadu, India
AU - Vadivel Sivalingam
AU - Shanmugam Muruganandham
AU - Sankar Karuppaiyan
AU - Mayakannan Ayyanar
Y1 - 2025/09/15
PY - 2025
N1 - https://doi.org/10.11648/j.sjph.20251305.11
DO - 10.11648/j.sjph.20251305.11
T2 - Science Journal of Public Health
JF - Science Journal of Public Health
JO - Science Journal of Public Health
SP - 244
EP - 256
PB - Science Publishing Group
SN - 2328-7950
UR - https://doi.org/10.11648/j.sjph.20251305.11
AB - Introduction: Infertility is an increasing public health concern in India, affecting approximately 27.5 million couples. Among women, infertility is frequently accompanied by psychosocial stress, societal stigma, and marital conflict, particularly in cultural settings where motherhood is closely linked to feminine identity. Despite technological advances in reproductive medicine, there is limited research examining the combined impact of biological, psychological, and social factors on female infertility and associated health issues. Objectives: This study aims to identify physical, psychological, and relational causes of infertility among women in Tamil Nadu. It also examines the effect of these factors on women's general and mental health. Methods: A purposive sample of 1,200 infertile women aged 18-50 years was selected from fertility centers in Thanjavur and Kumbakonam. Data was collected through structured questionnaires and analyzed using AMOS regression modelling. Fifteen hypotheses were tested to assess relationships among physical health conditions, psychosocial variables, and infertility-related health outcomes. Results: Major physical problems, specifically ovarian cysts (15.2%), thyroid disorders (14.9%), irregular menstruation (10%), and uterine fibroids (8.9%). Significant psychological impacts were observed from couple separation and negative spousal behavior (p Conclusion: Infertility in women is a multidimensional issue influenced by physical, psychological, and social factors. Integrating mental health care and relationship counselling into fertility treatment is essential for comprehensive care.
VL - 13
IS - 5
ER -
Copy
|
Download